
 |
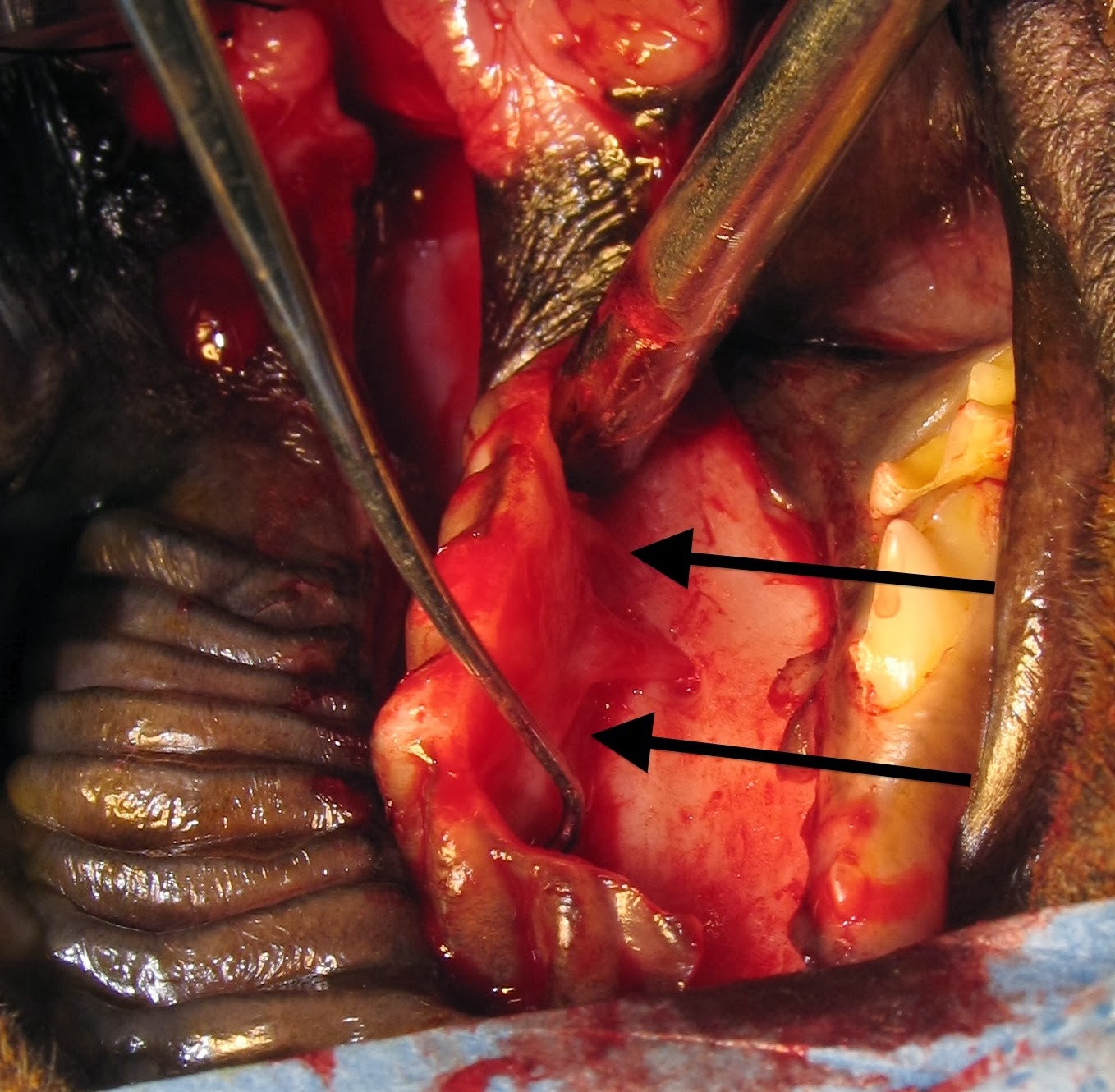
| Fig. 1: Cleft hard palate (yellow arrow) and soft palate (red arrow) in a dog. |
Congenital or acquired cleft
palates are seen commonly in dogs and cats. (Fig. 1) Puppies and kittens should
be checked for these defects immediately after birth. Early signs of cleft
palate are regurgitation of food and water into the nose. Aspiration pneumonia
can develop as a consequence. Clefts can involve the lips (primary) or hard and
soft palate (secondary). Most clefts require surgical repair but dehiscence is
common and some cases require multiple surgeries to achieve complete closure.
Principles of cleft palate repair:
Thoroughly evaluate the
animal for rhinitis and aspiration pneumonia. Treat appropriately prior to
surgery.
Preserve blood supply. The
major palatine artery supplies the soft tissues of the hard palate and should
be kept intact whenever possible.
Handle tissues gently. Use
stay sutures on edges of mucosa and flaps to avoid excessive trauma.
Use fine, absorbable
sutures. I prefer 4-0 polydioxanone since it has high tensile strength, is delayed
absorbable, and is monofilament.
Avoid having sutures knots
in the defect.
When making mucosal flaps to
repair defects, make them as large as possible to avoid tension across the
incision line.
Consider some kind of
implant material when local tissues are not adequate for a tension free
closure. (see future blog for an example)
Use an esophagostomy or
gastrostomy tube postoperatively to bypass the mouth for nutrition to avoid
food accumulation on the repaired palate.
Closure Technique
For most midline cleft
palate the mucoperiosteal flap technique is an effective technique for closure.
 |
| Fig. 2: Mucoperiosteal flap repair of a cleft hard palate in a dog. A: dotted lines indicate incisions to make the flap and elevate the mucosa on the opposite side; B: elevating the flap from the bone with a periosteal elevator; C: the flap has been inverted and sutured in place. Inset shows the horizontal mattress suture pattern from the edge of the flap to the overlying mucosa. (from: Marretta SM. Dentistry and diseases of the oropharynx. In: Saunders Manual of Small Animal Practice, editors Birchard and Sherding, 3rd edition, Elsevier, 2006, pg 609) |
(Fig. 3) A large rectangular flap is made on one side of the cleft using a
scalpel and periosteal elevator and is inverted.
 |
| Fig. 3: The flap has been elevated and is being inverted to the other side (arrows). |
This flap is tucked
underneath the mucosa on the other side. Again using the scalpel and
periosteal elevator, the mucoperiosteal tissues are elevated from the bone on
the side opposite from the flap to allow the flap to be tucked into the space
between the bone and the soft tissues. Use a horizontal mattress suture pattern
to close the flap over the defect. (Figs. 2 and 4)
 |
| Fig. 4: the flap has been inverted from right to left, tucked under the mucosa and sutured. The soft palate cleft was closed by splitting the soft tissue layer on each side with a scalpel to separate the oral mucosal side from the nasal mucosal side and sutured in 2 layers. |
The denuded bone where the
mucoperiosteal flap was harvested will become covered with granulation tissue and
then mucosa in a few weeks. (Fig. 5)
 |
| Fig. 5: 2 weeks postoperatively after mucoperiosteal flap repair |
Postoperative Care
Postoperatively, as
mentioned in the above principles, feed the animal through an esophagostomy or
gastrostomy tube to avoid food accumulation on the incision. Recheck the patient in 10-14 days to
ensure progression of normal healing.
J Am Vet Med Assoc. 1974 Aug 15;165(4):352-4.
,
References
Howard DR, et.al. Mucoperiosteal flap technique for cleft palate repair in dogs.J Am Vet Med Assoc. 1974 Aug 15;165(4):352-4.
No comments:
Post a Comment